The Ladder Behind Better Wound Outcomes
A Practical Guide to the Reconstructive Ladder for Wound Care Clinicians
By Ned Swanson, MD, President & Chief Medical Officer, PolarityBio
Chronic wounds are complex, and even with attentive care, outcomes can stall when the plan doesn’t match the biology, mechanics, and risk in front of you.
For plastic and reconstructive surgeons, one of the most useful mental frameworks for approaching wounds, acute or chronic, is the reconstructive ladder (1-3). While the concept is foundational in plastic surgery training, it's also incredibly relevant to all wound care professionals: podiatry, vascular surgery, general surgery, dermatology, advanced practice providers, and wound clinicians and nurses alike. As modern wound care teams become multidisciplinary, this framework can help with communication and transitions of care to offer patients comprehensive plans for their difficult wounds.
This blog is a practical, high-level guide to what the ladder is, how clinicians use it in real cases, and where today’s “in-between” wounds fit in modern wound care.
What Is the Reconstructive Ladder?
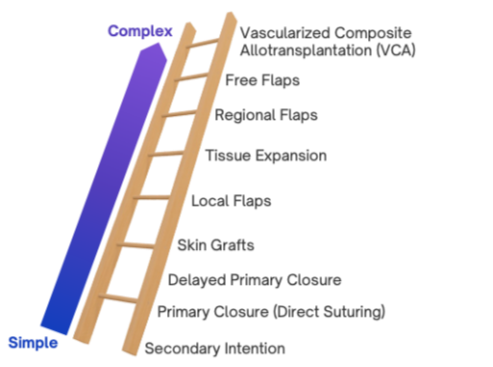
The reconstructive ladder is a conceptual framework that organizes wound closure strategies from simplest to most complex. It encourages clinicians to consider lower-risk, lower-complexity options first, and to “climb” only as needed based on wound characteristics and patient factors.
Importantly, it is not a rigid rulebook. It’s a way of thinking about a wound therapy plan that balances biology, mechanics, risk, and outcomes. At its core, the ladder helps clinicians answer a single question:
What is the safest, simplest, and most logical intervention that can reliably restore durable tissue coverage and function for this wound?
How the Ladder Is Used in Practice
When evaluating a wound, clinicians assess:
Depth
Size
Tissue quality
Vascularity
Bioburden and chronicity
Exposed avascular structures
Mechanical forces
Edema
Drainage
Patient comorbidities
The reconstructive ladder helps consolidate these variables to an appropriate intervention taking a step-wise approach from lower to higher complexity options and avoiding approaches that are unlikely to succeed.
The Main Rungs of the Reconstructive Ladder
Below is a simplified walkthrough of the classic ladder, from bottom to top.
1. Healing by Secondary Intention
Wounds are left open to heal naturally through granulation and epithelialization
Appropriate for small, superficial, well-vascularized wounds, focusing on lowering bioburden and a wound care plan that patients understand and can implement
Often slow and unpredictable in chronic wounds
Pros: Minimal intervention
Cons: Prolonged healing time, risk of breakdown, scarring
2. Primary Closure (Direct Suturing)
Direct suturing of wound edges
Requires minimal tension and healthy surrounding tissue
Pros: Fast, simple
Cons: Often not feasible in acute wounds without enough skin laxity, not for chronic wounds
3. Delayed Primary Closure
The wound is initially left open, often for bioburden/contamination control or optimization, and closed later.
Common in traumatic or infected wounds
Allows reassessment of tissue viability
Pros: Balances infection control with definitive closure, and patients can be medically optimized for healing success
Cons: Requires careful timing and wound management
4. Skin Grafts
Split-thickness skin grafts (STSGs) or full-thickness skin grafts (FTSGs)
Requires a well-prepared wound bed (clean, well-vascularized, minimal drainage, edema controlled)
Pros: STSGs provide reliable surface coverage
Cons: STSGs lack dermal appendages, contract, fragile, limited durability in high-stress areas, donor site morbidity
We’ve discussed the ins and outs of grafts in our recent Polarity Perspective blogs if you’d like to go deeper.
5. Local Flaps
Adjacent tissue is mobilized and rotated or advanced into the defect while maintaining its blood supply.
Provides more robust coverage with full-thickness and pliable skin
Requires a well-prepared wound bed
Pros: Better durability and tissue match
Cons: Increased surgical complexity and donor-site considerations
6. Tissue Expansion
Gradual expansion of nearby tissue using an implanted expander to generate additional skin for local coverage.
Common in reconstructive and staged procedures
Pros: Like-for-like tissue replacement
Cons: Time-intensive, requires multiple procedures, and can introduce implant complications (infection, migration, extrusion)
7. Regional or Pedicled Flaps
Transfer of tissue from a nearby anatomical region with a known vascular pedicle.
Useful for larger or more complex defects
Pros: Reliable blood supply, durable coverage
Cons: More invasive, limited by anatomy and reach, donor site morbidity
8. Free Flaps
Microsurgical transfer of tissue from a distant site with vascular anastomosis.
Reserved for complex, limb-threatening, or large defects
Pros: Powerful reconstructive option
Cons: High resource utilization, surgical risk, limited scalability
9. Vascularized Composite Allotransplantation (VCA)
Transplantation of complex, multi-tissue structures, such as skin, muscle, bone, nerves, and vessels, from a donor.
Includes procedures like hand or face transplantation
Pros: Restoration of complex anatomy and function not achievable by conventional reconstruction
Cons: Lifelong immunosuppression, ethical considerations, and currently limited indications
VCA represents the absolute top of the reconstructive ladder, reserved for the most severe tissue loss where no autologous option can restore form and function. Not a consideration for common chronic wounds.
Why This Matters in Chronic Wound Care
Many chronic wounds, including diabetic foot ulcers, arterial ulcers, venous leg ulcers, and pressure injuries, stall between rungs of the ladder. They are too complex for simple dressings but do not warrant, cannot tolerate, or are poor candidates for major reconstructive surgery.
This “middle ground” is where modern regenerative strategies become particularly relevant: therapies designed to restore normal wound biology, rather than simply cover defects.
Beyond the Ladder: The Reconstructive Elevator
Modern reconstruction has evolved beyond a strictly linear ladder into what’s often called the reconstructive elevator (1-3).
Instead of climbing rung by rung, the clinician can design a wound plan that:
Assesses the wound comprehensively
Selects the right level of intervention from the start
Moves directly to that option when indicated
This reflects a more nuanced understanding of:
Wound biology
Regenerative capacity
Patient-specific risk
Durability of outcomes
In other words, the goal is not to use the simplest option, but the most appropriate one for a customized-solution to a given patient case.
Final Thoughts
The reconstructive ladder is less about hierarchy and more about judgment based on principles. It provides a shared language across specialties and a framework for thoughtful escalation of care.
As wound care continues to evolve, especially with advances in tissue engineering as well as autologous regenerative therapies, the ladder, and the elevator, remain essential tools for matching the right biology to the right wound at the right time.
When we align technique with tissue biology, healing stops being incremental and becomes transformative.
The ultimate goal for patients is a wound-free life.
Achieving this goal is a journey, and this journey benefits from understanding and implementing reconstructive principles.
This was a review of the classic ladder focused on autologous reconstruction. There are many nuances to the reconstructive ladder that incorporate regenerative therapies and other advanced wound healing modalities (4-5). By no means is this overview comprehensive, and we will explore more details in subsequent articles.
References and Suggested Readings:
1. Buchanan, P. , Kung, T. & Cederna, P. (2016). Evidence-Based Medicine: Wound Closure. Plastic and Reconstructive Surgery, 138 (3S), 257S-270S. doi: 10.1097/PRS.00000000000027751.
2. Gottlieb LJ, Krieger LM. From the reconstructive ladder to the reconstructive elevator. Plast Reconstr Surg. 1994;93:1503–1504.
3. Janis JE, Kwon RK, Attinger CE. The new reconstructive ladder: modifications to the traditional model. Plast Reconstr Surg. 2011 Jan;127 Suppl 1:205S-212S. doi: 10.1097/PRS.0b013e318201271c. Erratum in: Plast Reconstr Surg. 2020 Nov;146(5):1212. doi: 10.1097/PRS.0000000000007512. PMID: 21200292.
4. De Francesco F, Zingaretti N, Parodi PC, Riccio M. The Evolution of Current Concept of the Reconstructive Ladder in Plastic Surgery: The Emerging Role of Translational Medicine. Cells. 2023 Nov 3;12(21):2567. doi: 10.3390/cells12212567. PMID: 37947645; PMCID: PMC10649097.
5. Grosu-Bularda A, Hodea FV, Cretu A, Lita FF, Bordeanu-Diaconescu EM, Vancea CV, Lascar I, Popescu SA. Reconstructive Paradigms: A Problem-Solving Approach in Complex Tissue Defects. J Clin Med. 2024 Mar 17;13(6):1728. doi: 10.3390/jcm13061728. PMID: 38541953; PMCID: PMC10971357.