Diabetic Foot Ulcers by the Numbers: Key Statistics Every Clinician Should Know
For this Polarity Perspective, we developed a resource for the key facts on DFUs:
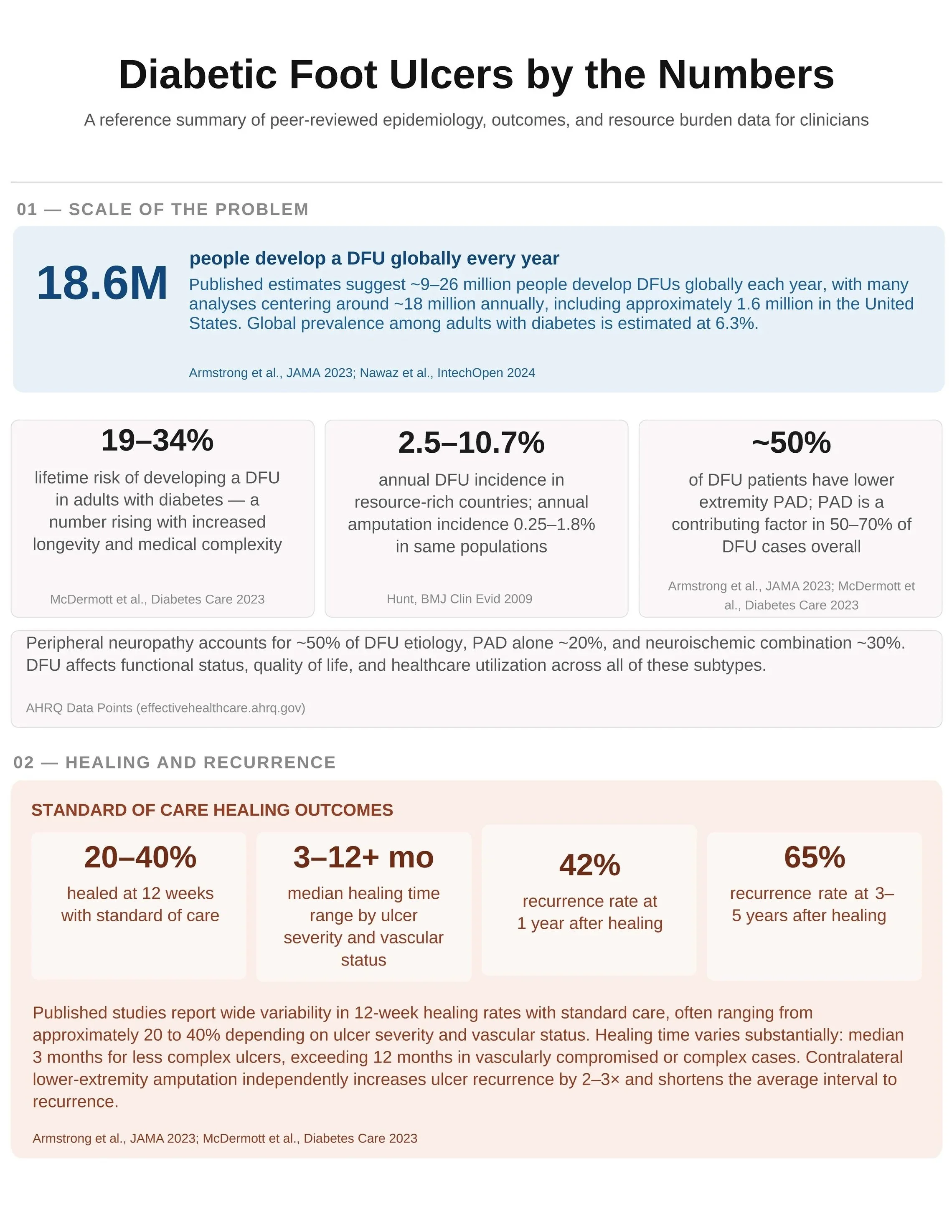
The Massive Scale of Diabetic Foot Ulcers
Lifetime Risk and Annual Incidence of DFUs
Healing Rates and Recurrence Statistics
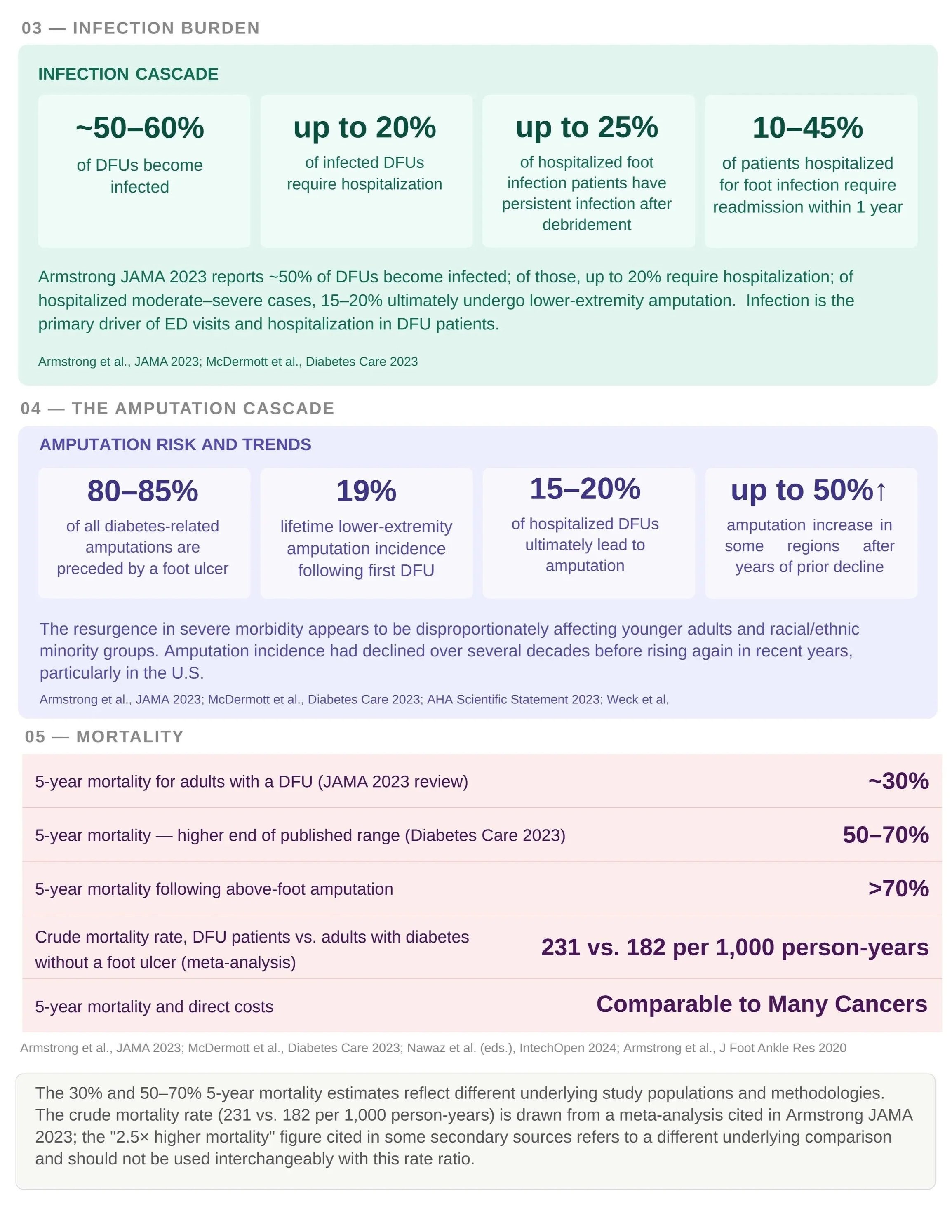
Infection, Hospitalization, and Amputation Cascade
The High Mortality Rate of Diabetic Foot Ulcers
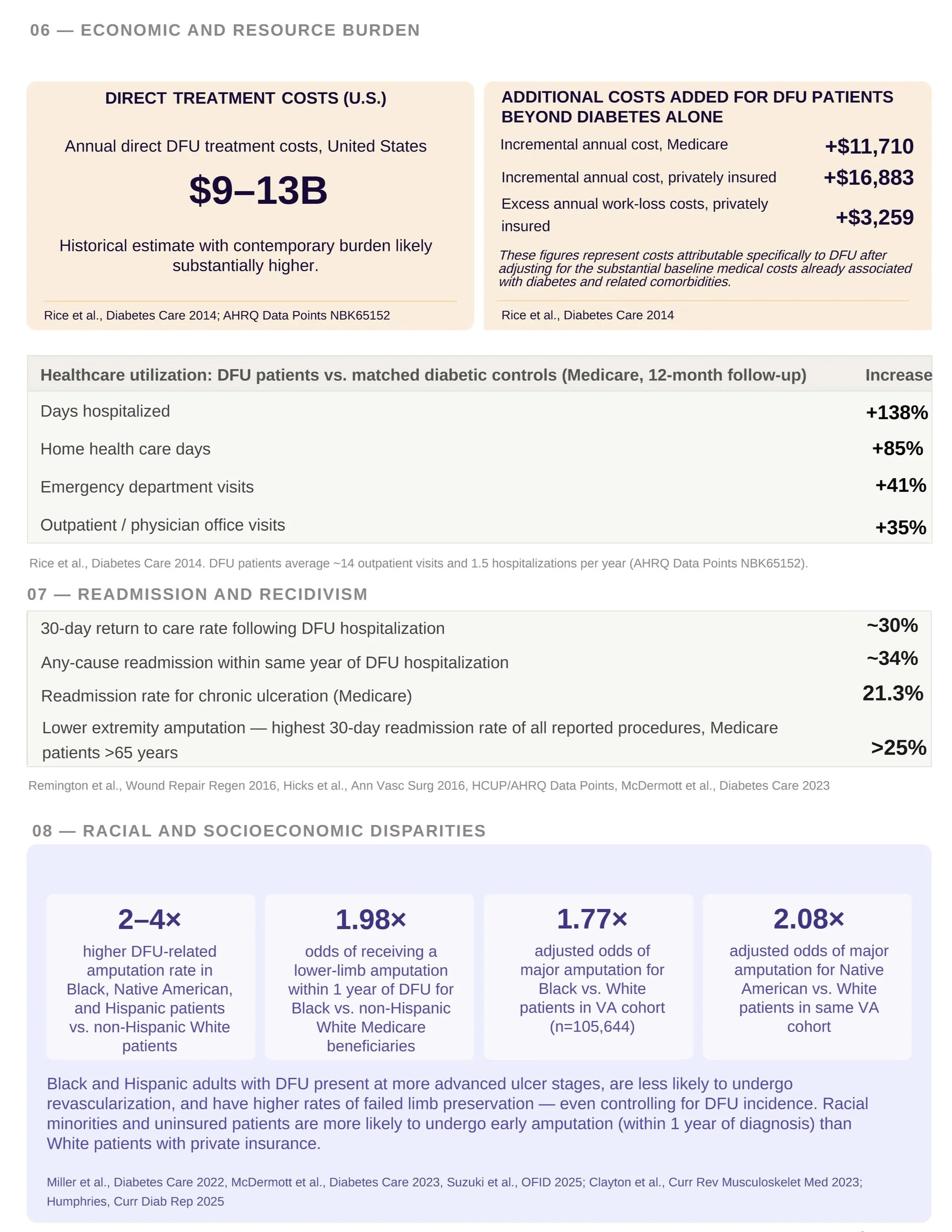
Economic and Resource Burden in the United States
Racial and Socioeconomic Disparities in DFU Outcomes
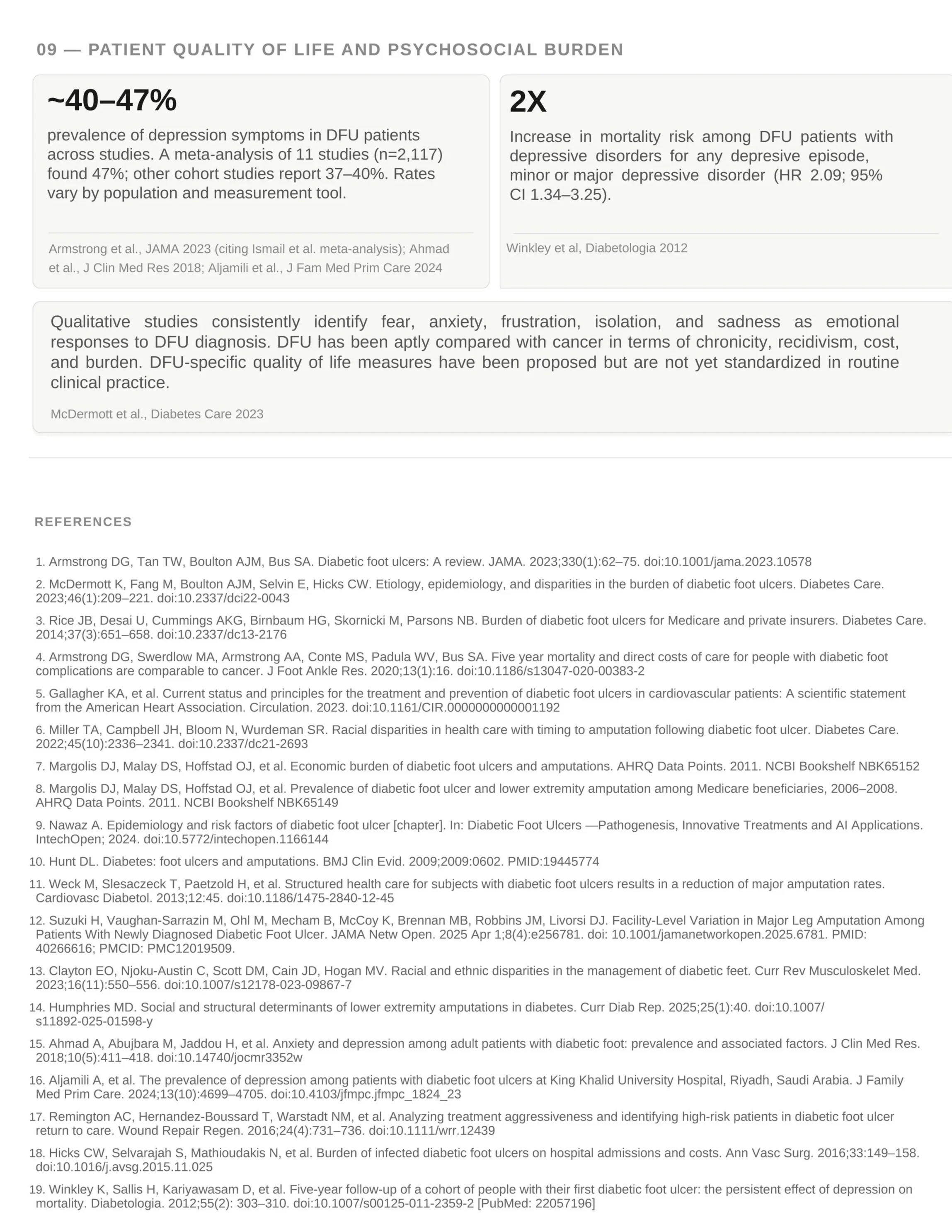
Mental Health Impact: Depression and Quality of Life
What These Numbers Mean for Prevention and Care
Key Diabetic Foot Ulcer Statistics Summary: While the infographic and article provide additional context, the table below consolidates the most important diabetic foot ulcer statistics into a single, easy-to-reference resource.
Diabetic Foot Ulcers by the Numbers
A reference summary of peer-reviewed epidemiology, outcomes, and resource-burden data for clinicians.
Source: PolarityBio “DFU By The Numbers.” Figures reflect published peer-reviewed literature; full citations below.
| Metric | Figure | Context / detail | Source(s) |
|---|---|---|---|
| 01 — Scale of the Problem | |||
| People who develop a DFU globally every year | 18.6M | Published estimates suggest ~9–26 million people develop DFUs globally each year, with many analyses centering around ~18 million annually, including ~1.6 million in the United States. Global prevalence among adults with diabetes ≈ 6.3%. | Armstrong et al., JAMA 2023; Nawaz et al., IntechOpen 2024 |
| Lifetime risk of developing a DFU (adults with diabetes) | 19–34% | Rising with increased longevity and medical complexity. | McDermott et al., Diabetes Care 2023 |
| Annual DFU incidence (resource-rich countries) | 2.5–10.7% | Annual amputation incidence 0.25–1.8% in same populations. | Hunt, BMJ Clin Evid 2009 |
| DFU patients with lower-extremity PAD | ~50% | PAD is a contributing factor in 50–70% of DFU cases overall. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 |
| Etiology breakdown (note) | — | Peripheral neuropathy accounts for ~50% of DFU etiology, PAD alone ~20%, and neuroischemic combination ~30%. | AHRQ Data Points (effectivehealthcare.ahrq.gov) |
| 02 — Healing and Recurrence (standard-of-care outcomes) | |||
| Healed at 12 weeks with standard of care | 20–40% | Wide variability depending on ulcer severity and vascular status. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 |
| Median healing time range | 3–12+ mo | Median ~3 months for less complex ulcers; exceeding 12 months in vascularly compromised or complex cases. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 |
| Recurrence rate at 1 year after healing | 42% | Contralateral lower-extremity amputation independently increases ulcer recurrence by 2–3× and shortens the interval to recurrence. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 |
| Recurrence rate at 3–5 years after healing | 65% | See note on contralateral amputation above. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 |
| 03 — Infection Burden (infection cascade) | |||
| DFUs that become infected | ~50–60% | Infection is the primary driver of ED visits and hospitalization in DFU patients. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 |
| Infected DFUs requiring hospitalization | up to 20% | Of hospitalized moderate–severe cases, 15–20% ultimately undergo lower-extremity amputation. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 |
| Hospitalized foot-infection patients with persistent infection after debridement | up to 25% | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 | |
| Patients hospitalized for foot infection requiring readmission within 1 year | 10–45% | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023 | |
| 04 — The Amputation Cascade (risk and trends) | |||
| Diabetes-related amputations preceded by a foot ulcer | 80–85% | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023; AHA Scientific Statement 2023; Weck et al. | |
| Lifetime lower-extremity amputation incidence following first DFU | 19% | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023; AHA Scientific Statement 2023; Weck et al. | |
| Hospitalized DFUs that ultimately lead to amputation | 15–20% | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023; AHA Scientific Statement 2023; Weck et al. | |
| Amputation increase in some regions after years of prior decline | up to 50% ↑ | Resurgence disproportionately affects younger adults and racial/ethnic minority groups. | Armstrong et al., JAMA 2023; McDermott et al., Diabetes Care 2023; AHA Scientific Statement 2023; Weck et al. |
| 05 — Mortality | |||
| 5-year mortality for adults with a DFU (JAMA 2023 review) | ~30% | The 30% and 50–70% estimates reflect different study populations and methodologies. | Armstrong et al., JAMA 2023 |
| 5-year mortality — higher end of published range | 50–70% | McDermott et al., Diabetes Care 2023 | |
| 5-year mortality following above-foot amputation | >70% | Nawaz et al. (eds.), IntechOpen 2024 | |
| Crude mortality rate: DFU patients vs. adults with diabetes without a foot ulcer (meta-analysis) | 231 vs. 182 / 1,000 person-years | The “2.5× higher mortality” figure in some secondary sources refers to a different comparison and should not be used interchangeably with this rate ratio. | Armstrong et al., JAMA 2023; Armstrong et al., J Foot Ankle Res 2020 |
| 5-year mortality and direct costs | Comparable to many cancers | Armstrong et al., J Foot Ankle Res 2020 | |
| 06 — Economic and Resource Burden (U.S.) | |||
| Annual direct DFU treatment costs, United States | $9–13B | Historical estimate; contemporary burden likely substantially higher. | Rice et al., Diabetes Care 2014; AHRQ Data Points NBK65152 |
| Incremental annual cost, Medicare (beyond diabetes alone) | +$11,710 | Costs attributable specifically to DFU after adjusting for baseline diabetes-related costs. | Rice et al., Diabetes Care 2014 |
| Incremental annual cost, privately insured (beyond diabetes alone) | +$16,883 | As above. | Rice et al., Diabetes Care 2014 |
| Excess annual work-loss costs, privately insured | +$3,259 | DFU patients average ~14 outpatient visits and 1.5 hospitalizations per year. | Rice et al., Diabetes Care 2014; AHRQ Data Points NBK65152 |
| Healthcare utilization vs. matched diabetic controls — days hospitalized (Medicare, 12-mo) | +138% | Rice et al., Diabetes Care 2014 | |
| Healthcare utilization — home health-care days | +85% | Rice et al., Diabetes Care 2014 | |
| Healthcare utilization — emergency department visits | +41% | Rice et al., Diabetes Care 2014 | |
| Healthcare utilization — outpatient / physician office visits | +35% | Rice et al., Diabetes Care 2014 | |
| 07 — Readmission and Recidivism | |||
| 30-day return-to-care rate following DFU hospitalization | ~30% | Remington et al., 2016; Hicks et al., 2016; HCUP/AHRQ; McDermott et al., Diabetes Care 2023 | |
| Any-cause readmission within same year of DFU hospitalization | ~34% | Remington et al., 2016; Hicks et al., 2016; HCUP/AHRQ; McDermott et al., Diabetes Care 2023 | |
| Readmission rate for chronic ulceration (Medicare) | 21.3% | Remington et al., 2016; Hicks et al., 2016; HCUP/AHRQ; McDermott et al., Diabetes Care 2023 | |
| Lower-extremity amputation — highest 30-day readmission rate of all reported procedures (Medicare >65 yrs) | >25% | Remington et al., 2016; Hicks et al., 2016; HCUP/AHRQ; McDermott et al., Diabetes Care 2023 | |
| 08 — Racial and Socioeconomic Disparities | |||
| Higher DFU-related amputation rate: Black, Native American, Hispanic vs. non-Hispanic White | 2–4× | Minority and uninsured patients present at more advanced ulcer stages and are more likely to undergo early amputation. | Miller et al., 2022; McDermott et al., 2023; Suzuki et al., 2025; Clayton et al., 2023; Humphries, 2025 |
| Odds of lower-limb amputation within 1 yr of DFU: Black vs. non-Hispanic White Medicare beneficiaries | 1.98× | Miller et al., 2022; McDermott et al., 2023; Suzuki et al., 2025; Clayton et al., 2023; Humphries, 2025 | |
| Adjusted odds of major amputation: Black vs. White, VA cohort (n=105,644) | 1.77× | Miller et al., 2022; McDermott et al., 2023; Suzuki et al., 2025; Clayton et al., 2023; Humphries, 2025 | |
| Adjusted odds of major amputation: Native American vs. White, same VA cohort | 2.08× | Miller et al., 2022; McDermott et al., 2023; Suzuki et al., 2025; Clayton et al., 2023; Humphries, 2025 | |
| 09 — Patient Quality of Life and Psychosocial Burden | |||
| Prevalence of depression symptoms in DFU patients | ~40–47% | Meta-analysis of 11 studies (n=2,117) found 47%; other cohort studies report 37–40%. Rates vary by population and tool. | Armstrong et al., JAMA 2023 (citing Ismail et al.); Ahmad et al., 2018; Aljamili et al., 2024 |
| Increase in mortality risk among DFU patients with depressive disorders | 2× | Any depressive episode, minor or major (HR 2.09; 95% CI 1.34–3.25). | Winkley et al., Diabetologia 2012 |
References
- Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic foot ulcers: A review. JAMA. 2023;330(1):62–75.
- McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209–221.
- Rice JB, et al. Burden of diabetic foot ulcers for Medicare and private insurers. Diabetes Care. 2014;37(3):651–658.
- Armstrong DG, et al. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16.
- Gallagher KA, et al. AHA scientific statement on treatment and prevention of DFUs in cardiovascular patients. Circulation. 2023.
- Miller TA, et al. Racial disparities in health care with timing to amputation following diabetic foot ulcer. Diabetes Care. 2022;45(10):2336–2341.
- Margolis DJ, et al. Economic burden of diabetic foot ulcers and amputations. AHRQ Data Points. 2011. NBK65152.
- Margolis DJ, et al. Prevalence of DFU and lower extremity amputation among Medicare beneficiaries, 2006–2008. AHRQ Data Points. 2011. NBK65149.
- Nawaz A. Epidemiology and risk factors of diabetic foot ulcer. In: Diabetic Foot Ulcers — Pathogenesis, Innovative Treatments and AI Applications. IntechOpen; 2024.
- Hunt DL. Diabetes: foot ulcers and amputations. BMJ Clin Evid. 2009;2009:0602.
- Weck M, et al. Structured health care for subjects with DFUs reduces major amputation rates. Cardiovasc Diabetol. 2013;12:45.
- Suzuki H, et al. Facility-level variation in major leg amputation among patients with newly diagnosed DFU. JAMA Netw Open. 2025;8(4):e256781.
- Clayton EO, et al. Racial and ethnic disparities in the management of diabetic feet. Curr Rev Musculoskelet Med. 2023;16(11):550–556.
- Humphries MD. Social and structural determinants of lower extremity amputations in diabetes. Curr Diab Rep. 2025;25(1):40.
- Ahmad A, et al. Anxiety and depression among adult patients with diabetic foot. J Clin Med Res. 2018;10(5):411–418.
- Aljamili A, et al. Prevalence of depression among patients with DFUs, Riyadh. J Family Med Prim Care. 2024;13(10):4699–4705.
- Remington AC, et al. Treatment aggressiveness and high-risk patients in DFU return to care. Wound Repair Regen. 2016;24(4):731–736.
- Hicks CW, et al. Burden of infected diabetic foot ulcers on hospital admissions and costs. Ann Vasc Surg. 2016;33:149–158.
- Winkley K, et al. Five-year follow-up of people with their first DFU: persistent effect of depression on mortality. Diabetologia. 2012;55(2):303–310.